







Enhanced cognitive behavioral therapy (CBT-E) was developed to improve outcomes for the treatment of eating disorders. Based on the transdiagnostic theory of eating disorders created by Christopher Fairburn, Zafra Cooper and Roz Shafran, CBT-E is the leading treatment for eating disorders.1 It has a high rate of success with two-thirds of patients experiencing long-term improvements in their eating disorder symptoms.2,3,4
Eating Disorder Treatment That Works – Delivered At Home
Eating disorder treatment is hard – which is why you shouldn’t have to do it alone. Equip provides compassionate, evidence-based virtual treatment that supports you every step of the way, and allows you to recover at home without pressing pause on your life. Covered by insurance.
What Is CBT-E?
CBT-E is a form of cognitive behavioral therapy (CBT) that focuses on addressing, disrupting, and modifying the factors that maintain someone’s eating disorder. It is a time-limited and structured treatment. CBT-E uses psychoeducation and cognitive and behavioral strategies and techniques.
How Does CBT-E Work?
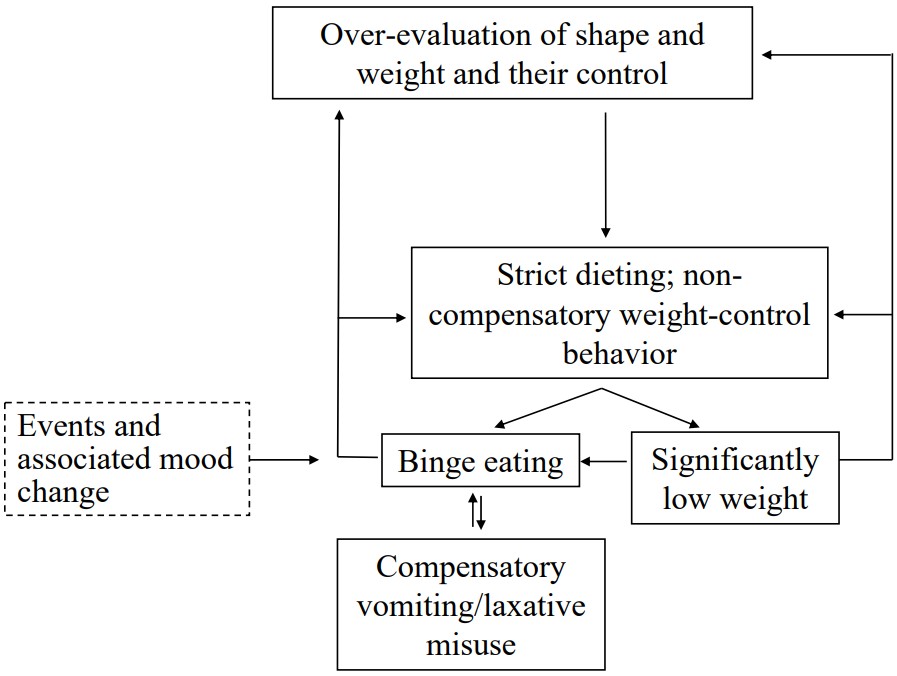
CBT-E emphasizes the need for a collaborative relationship between the patient and therapist in order to overcome the eating disorder. CBT-E focuses on the factors that maintain the eating disorder by creating a personalized formulation of the factors underlying the illness. Each formulation is tailored based on the symptoms, core reasons for the disorder, and triggers that are relevant to the patients.
Similar to other CBT treatments, CBT-E utilizes:
- Psychoeducation
- Self-monitoring records
- Homework
- Implementation of techniques
- Cognitive restructuring
- Problem-solving skills
CBT-E Treatment Timeline
CBT-E typically starts with one evaluation session that is 1.5-2 hours followed by twenty 50-minute therapy sessions over the course of twenty weeks. The first eight sessions occur twice a week, then the next ten sessions are weekly, and the last three sessions are every other week.
Some patients may require a 40-session version (like patients who are underweight or are diagnosed with anorexia nervosa), but the 20-session version is appropriate for over 80% of adult outpatients.3
What Is CBT-E For Eating Disorders Used to Treat?
CBT-E is suitable for patients with all forms of eating disorders, including binge eating disorder, anorexia nervosa, and bulimia nervosa. Patients who are underweight or have a diagnosis of anorexia nervosa will likely require the longer, more intense version of CBT-E.
How Can CBT-E Help With Eating Disorders?
CBT-E allows people with eating disorders to learn about how their disorder functions, how it is maintained, and how to disrupt the self-reinforcing cycle that maintains the eating disorder.3 It also provides them with psychoeducation about their eating disorders and their health, which helps to combat distorted beliefs that fuel their eating disorder.3,5
Concerned About An Eating Disorder?
If thoughts about food or your body are starting to cause daily stress, it’s well worth taking a closer look. Equip offers a free, confidential eating disorder screener to help you determine what’s going on and decide next steps.
4 Stages of CBT-E
CBT-E is a time-limited, tailored treatment that helps the patient to understand, break down and disrupt the self-reinforcing cycle of their eating disorder. The treatment utilizes homework, skills, and tools to increase the person’s awareness of the connection between their thoughts, feelings, and behaviors and to help the patient modify their reactions to certain events and triggers.
Here are the four stages of CBT-E:3
1. Starting Well
Stage one is the intensive initial stage when the patient meets with a therapist twice a week. These sessions provide the groundwork for the treatment where information is gathered about the patient’s disorder. Then, a formulation is developed and the utility of the formulation is described to the patient. The structure of sessions is introduced and explained and homework is introduced.
Stage one of CBT-E will include:
- Understanding the Disorder: The therapist and patient explore the nature and severity of the patient’s eating disorder. The therapist helps to engage patient in treatment and create change. Collaboratively, the therapist and patient analyze factors that maintain the eating disorder’s self-reinforcing cycle.
- Weekly Weigh-Ins: Weekly weigh-ins are used to help the patient understand natural fluctuations in weight and weight trends, which are plotted on a graph. The patient is asked not to weigh themselves outside of treatment.
- Self-Monitoring Records: The therapist explains self-monitoring records, which are forms used by patients to record everything that they eat or drink and their thoughts and feelings during those times. The patient also documents any excessive consumption of food or drink, incidents of vomiting, and use of laxatives or diuretics, as well as other compensatory behaviors in reaction to eating on the self-monitoring records. Self-monitoring forms enhance self-awareness surrounding eating behaviors and when they occur.
- Regular Eating Intervals: The patient is instructed to eat in regular intervals—three meals a day and three snacks—while avoiding eating between meals or exceeding four hours without eating. Style of eating (e.g, abnormal pace of eating, eating while doing other activities, grazing), purging, feelings of fullness, low weight, or excessive exercise are addressed and explored through self-monitoring.
2. Taking Stock
Stage two is a transitional stage of treatment, which consists of 1-2 sessions.
During stage two of CBT-E, the goals are to:
- Review the progress in treatment collaboratively
- Identify barriers to creating change: Examples include fear of change, resistance to change, competing demands (not prioritizing treatment), interpersonal difficulties or life challenges, depression, severe low self-esteem, perfectionism, misusing substances, or poor planning.
- Review and modify formulation: Over the course of several weeks of self-monitoring, for example, someone who previously thought she only binge ate in reaction to breaking a dietary rule may notice that whenever she feels sad or stressed she also binge eats. She then would need to add “mood changes” (i.e., feeling sad or stressed) as a trigger for binge eating to her formulation.
- Decide whether to use a broad or focused version of CBT-E: Typically, the focused version of CBT-E is implemented as it is less challenging and more effective than the broad version. The broad version is for patients whose eating disorder is maintained by clinical perfectionism, core low self-esteem, and interpersonal problems.
- Design the main portion of treatment in Stage 3: Based on the patient’s needs and presentation, the clinician and patient decide which mechanisms to address and in what order. Once this strategy is decided the plan is set for stage three.
3. Addressing Maintaining Factors
The plan developed in stage two is carried out in stage three. The plan for stage three will remain flexible and will be modified should there be any changes to the maintaining factors of the eating disorder.
The elements that might be addressed in stage three of CBT-E include:
- Identifying versus evaluating body shape, weight, or control vs. eating and the consequences
- Exploring and focusing on the importance of other factors for self-evaluation
- Addressing body checking behaviors (i.e., mirror checking, comparing bodies, and body avoidance)
- Addressing feeling fat
- Identifying the origins of the over-evaluation
- Learning to identify and control the mindset surrounding the eating disorder, including having strategies for dealing with any relevant triggers
4. Ending Well
Stage four consists of three sessions that take place every other week. The primary focus of these sessions is the future. It is important for the person to be able to apply the skills learned in treatment on their own so they can take ownership of the progress made.
During this stage the patient and therapist will address:
- Reactions and concerns to the ending treatment
- Ways to maintain progress made in treatment
- Development of a short-term maintenance plan, which is what the patient will continue to work on until they have their review appointment in 20 weeks
- Reducing and phasing out of treatment procedures and homework, like self-monitoring and weekly weigh-ins
Graduation From Self-Monitoring
In week 18, the patient will stop self-monitoring records and in-session weigh-ins. The patient will begin to adjust to weighing themselves at home and become attuned to what is occurring throughout the day when they are eating or have the urge to engage in disordered eating behaviors (e.g., binge eating, purging, over-exercising).
Self-Identified Coping Strategies
The patient will identify strategies and aspects of treatment that could be implemented in their daily lives to prevent a relapse long-term. For example, a patient may continue to utilize monitoring records or implement them around high stress times, like the holidays.
Relapse Prevention & Maintenance Plans
The therapist will help the patient develop realistic expectations in case of setbacks. The patient and therapist identify triggering situations where the patient could encounter the return of the eating disorder mindset or behaviors. They will also identify the differences between a lapse and a relapse, ways to address setbacks when they occur, and when to seek help with a long-term maintenance plan.
Post-Treatment Review
The patient will also complete a post-treatment review, which will include taking an assessment to identify the present state of the eating disorder and whether it is interfering with the ability to function. Typically, the Eating Disorder Questionnaire and the Clinical Impairment Assessment Questionnaire are used.
The post-treatment review will also include:
- A review of the progress over the past 20 weeks
- A review of the short-term plan and how this will be implemented to address remaining eating disorder features and symptoms
- Identifying whether weekly weigh-ins should continue or whether a more flexible approach should be implemented
- Exploring ways to handle setbacks
- Reviewing and making necessary changes to the long-term maintenance plan
How to Find a CBT-E Specialist
There is no specific certification to become a CBT-E therapist, but when looking for a CBT-E therapist, it is important to know what to look for. Knowing what to expect in CBT-E treatment can also help ensure that you’re hiring a CBT therapist who is administering this protocol-based treatment.
Here is what to look for in a CBT-E specialist:
- Previous experience at a clinic or hospital that administers CBT-E
- Training in CBT-E and experience providing it
- Training and supervision by a CBT-E expert
The NEDA website allows you to search local hospitals that provide evidence-based treatments for eating disorders. You can also start your search for a therapist through an online therapist directory. There are also several online programs that provide help for eating disorders, like Equip Health.
Eating Disorder Treatment That Works – Delivered At Home
Eating disorder treatment is hard – which is why you shouldn’t have to do it alone. Equip provides compassionate, evidence-based virtual treatment that supports you every step of the way, and allows you to recover at home without pressing pause on your life. Covered by insurance.
Example of CBT-E
Lucy Smith is a 21-year-old female who lives alone. She has been struggling with dieting, food avoidance, binge eating, and purging (self-induced vomiting) since high school. She has been diagnosed with bulimia nervosa.
Lucy utilizes eating disorder behaviors to manage stress and challenging situations. She often has negative thoughts about her body, like “I have flabby arms and legs” and “I look terrible,” which fuels her restrictive eating behaviors (i.e., cutting out carbohydrates and skipping meals). Skipping meals results in her going long periods without eating, which places her at an increased risk for binge eating.
Lucy avoids certain foods like chips, cake, ice cream, popcorn, and donuts. She struggles to manage stressful events (e.g., disagreements with friends or family members which lead her to want to modify her feelings through binge eating and purging. Binge eating often results in self-induced vomiting in an effort to offset the calories consumed during the binge.
Binge eating also leads to more negative thoughts about herself, further reinforcing the cycle of her eating disorder. Lucy also weighs herself multiple times a week and evaluates herself based on weight change.
Example Treatment Plan
The patient’s plan will utilize self-monitoring records to help understand her eating disorder and how it functions, as well as to identify triggers. Lucy will also be encouraged to develop a formulation that explains the self-reinforcing vicious cycle of her disorder and why it is so difficult to modify her thoughts and behaviors.
Lucy will be introduced to weekly weigh-ins (no weigh-ins in between) and charting her weekly weight. Regular eating intervals will also be implemented (e.g., three meals a day and three snacks with no eating between meals and/or exceeding four hours without eating).3 If Lucy binge eats, she is instructed to return to regular eating immediately after.
Lucy will receive psychoeducation about eating disorders. Specifically, the health implications of EDs. For instance, ED behaviors can cause electrolyte imbalance, cardiac problems, and dental problems. Lucy would then begin addressing over-evaluations by understanding its consequences and developing new domains for self-evaluation.
Lucy then explores the risks and consequences associated with the way she evaluates herself (i.e., a majority of self-evaluations are based on her weight, shape, and ability to control her eating). Lucy is then encouraged to find other areas of her self-evaluation that are easy to enhance to reduce the importance of shape, weight, and eating behaviors.
Lucy will engage in new activities and re-engage with previous areas of interest in order to enhance areas of self-evaluation. To better understand her eating disorder, Lucy will explore its origins, looking at what occurred 12 months before and after the ED mindset started. Doing so will help her learn to identify the ED mindset, triggers, and how to disrupt or modify this type of thinking.
Lucy will also address dieting and restrictive eating and the ways in which these behaviors can be problematic. For example, dieting is problematic because it causes Lucy to focus her energy on food and eating vs. her work or other more fulfilling tasks. Diet also contributes to feelings of failing, guilts, and anxiety disorders.
Lucy would be encouraged to identify ways dietary restraint and restriction leads to binge eating. Going long periods of time without eating will physiologically increase the risk of a binge eating episode. Having dietary rules around foods or avoiding certain foods may cause Lucy to feel out of control or have a self-defeating attitude when she eats this food group or breaks a rule triggering a binge eating episode.
Lucy would also take daily notes of dietary rules and rule-breaking on self-monitoring records so she can see the consequences of this rule-breaking in real time. Lucy would be challenged to break rules purposefully in order to help dispute or modify these beliefs about what would occur if rules are broken, thus freeing her of these beliefs over time.
Food avoidance or feared foods would be addressed by having Lucy write down all the foods she avoids and systematically work through eating (exposing herself to them) and integrating them into her diet more regularly to disrupt beliefs and fears associated with these avoided foods.
7 Steps For Problem Solving
Lucy would also learn to develop problem solving skills for triggering events and mood-related triggers, utilizing seven steps for problem solving.3,5
Here are seven steps for problem solving:
- Identify the problem as soon as possible
- Specify the problem (i.e., the nature of the problem and if there is more than one to solve)
- Brainstorm as many solutions as possible
- Identify the pros and cons of the solutions
- Choose the best solution or combination of solutions
- Move forward with the solution
- Evaluate the problem-solving process by focusing on the process of solving the problem, not whether it was successful
Lucy has difficulty tolerating certain moods. In order to better understand Lucy’s mood intolerance, she would be asked to identify events that trigger shifts in mood and her thought processes surrounding them and how this leads to binge eating behaviors. Doing this will help Lucy learn about the impact of her appraisals of events on her mood.
She will observe how her thinking following events can leave her feeling overwhelmed or unable to manage a situation, which results in mood modulating behaviors (i.e., binge eating or other destructive behaviors) and further negative mood and negative thoughts about herself.3
Lucy will learn to observe and analyze her reactions to events and experiment with alternative responses. For example, she may alternatively respond by implementing problem solving (described above) and tolerating or accepting the mood (e.g., understanding that moods are part of the human experience and they will subside). Additionally, Lucy may learn that moods don’t require action and she can just “ride out” the uncomfortable mood.
Functional Ways to Change Mood
Lucy will also learn functional ways to change her mood, including listening to music, moving her body, or getting out into nature.
Here are functional ways to change mood:
- Putting on music that has a positive impact on mood or thoughts
- Reaching out to others for connection or support
- Taking a walk or exercising
- Taking a shower or bath
- Engaging in an activity outside of your home
Lucy might also try placing barriers to dysfunctional mood changing behaviors, such as being around other people so she won’t binge and purge or not going to the market when feeling the urge to binge. Lucy will then engage in stage four of treatment.
In My Experience
If you or a loved one is dealing with an eating disorder, seeking the help of a trained mental health professional who specializes in CBT-E could really help. Don’t wait to seek care if you are dealing with any form of disordered eating.

CBT-E Infographics
ChoosingTherapy.com strives to provide our readers with mental health content that is accurate and actionable. We have high standards for what can be cited within our articles. Acceptable sources include government agencies, universities and colleges, scholarly journals, industry and professional associations, and other high-integrity sources of mental health journalism. Learn more by reviewing our full editorial policy.
-
Fairburn CG, Cooper Z, Shafran R. Cognitive behaviour therapy for eating disorders: a “transdiagnostic” theory and treatment. Behav Res Ther. 2003 May;41(5):509-28. doi: 10.1016/s0005-7967(02)00088-8. PMID: 12711261.
-
Byrne, S. M., Fursland, A., Allen, K. L. and Watson, H. (2011). The effectiveness of enhanced cognitive behavioural therapy for eating disorders: an open trial. Behaviour Research and Therapy, 49, 219–226. doi: 10.1016/j.brat.2011.01.006
-
Fairburn, C. G. (2008). Cognitive behavioral therapy and eating disorders. New York, New York: Guilford Press.
-
CBT-E. (N.D.). The Current Status of CBT-E. Retrieved from: https://www.cbte.co/what-is-cbte/current-status-cbte/.
-
Fairburn, C. G. (2013). Overcoming binge eating: The proven program to learn why you binge and how you can stop (2nd ed.). Guilford Press.

We regularly update the articles on ChoosingTherapy.com to ensure we continue to reflect scientific consensus on the topics we cover, to incorporate new research into our articles, and to better answer our audience’s questions. When our content undergoes a significant revision, we summarize the changes that were made and the date on which they occurred. We also record the authors and medical reviewers who contributed to previous versions of the article. Read more about our editorial policies here.
Author: Gabrielle Schreyer-Hoffman, Ph.D. (No Change)
Reviewer: Naveed Saleh, MD, MS (No Change)
Primary Changes: Updated for readability and clarity. Reviewed and added relevant resources.
Author: Gabrielle Schreyer-Hoffman, Ph.D.
Reviewer: Naveed Saleh, MD, MS
Your Voice Matters
Can't find what you're looking for?
Request an article! Tell ChoosingTherapy.com’s editorial team what questions you have about mental health, emotional wellness, relationships, and parenting. Our licensed therapists are just waiting to cover new topics you care about!
Leave your feedback for our editors.
Share your feedback on this article with our editors. If there’s something we missed or something we could improve on, we’d love to hear it.
Our writers and editors love compliments, too. :)

Best Online Therapy Services
There are a number of factors to consider when trying to determine which online therapy platform is going to be the best fit for you. It’s important to be mindful of what each platform costs, the services they provide you with, their providers’ training and level of expertise, and several other important criteria.
Eating Disorders: Types, Treatments & How To Get Help
If you or a loved one are dealing with an eating disorder, know you’re not alone. Treatment can significantly help improve thought patterns and symptoms that can contribute to eating disorders, and having a robust care team can be an effective prevention strategy long-term.
