







Repetitive and ritualistic behaviors are a hallmark feature of both OCD and autism.1 While these diagnoses are understood as being unique in many ways, there is also considerable overlap in the way that symptoms impact people.2 Specifically, compulsions and rituals in both populations can serve to relieve or prevent underlying anxiety or distress.
Do I have OCD?
NOCD therapists can evaluate you for OCD and help you receive appropriate care. NOCD is covered by most major insurance plans. Get started with a free 15 minute call.
What Is Autism?
While presentations are incredibly varied from person to person, autism can be broadly characterized by core features in two areas–social communication and restricted and/or repetitive behaviors.1 Examples of features commonly attributed to autism include difficulties with shared imaginative play, insistence on sameness in routine, and repetitive motor movements (e.g., lining up toys, arm flapping). Autism can be diagnosed by a variety of different professionals, often following a clinical observation and caregiver interview.
Autism may be evident throughout childhood following delays in milestones (i.e. language development, social skills) or as the result of restricted interests that differ from same-aged peers.3 Many autistic children also present with co-occurring conditions such as speech delays, learning difficulties, restricted food choices, and gastrointestinal problems.3 Many of these coexisting problems are well addressed through various therapies, though they are not “treating” the underlying autism diagnosis, per se.
Just as the signs and symptoms of autism vary greatly, so too do the outcomes. Some autistic people grow up to live independently in the community, while others need more support from trained professionals.
What Is Obsessive Compulsive Disorder (OCD)?
Obsessive compulsive disorder (OCD) is diagnosed when people have recurring, unwanted, or distressing thoughts (obsessions) followed by ritualistic behaviors to try to manage the anxiety of the obsessions.1 Obsessive thoughts are often viewed as being intrusive and impair someone’s ability to function. In other words, the nature of these thoughts for people with OCD significantly interferes with their quality of life.
Compulsions can be visible to others, such as hand-washing or cleaning, or they can be harder to notice, such as counting or repeating specific words or phrases.4 Many people with OCD report tension or anxiety that only resolves once they’ve completed a compulsive behavior.
Is OCD Autism?
OCD is not a form of Autism, and it is not on the Autism spectrum. OCD is a mental health disorder that is closely linked with anxiety.5 Some research shows OCD is a form of neurodivergence. Autism diagnoses now encompass diagnoses that used to be considered separate, including Asperger’s syndrome, childhood disintegrative disorder, and an unspecified form of pervasive developmental disorder.6
How Do Symptoms of OCD and Autism Overlap?
At first glance, there can appear to be pretty significant overlap between autism and OCD. Symptoms of both conditions include the presence of some behaviors that may seem atypical. However, it is the individuals’ experience of these symptoms that can offer important evidence about how to differentiate them. Ultimately, these are unique disorders that require different levels of intervention and long-term support.
Restrictive-Repetitive Behaviors
Repetitive behaviors can include almost any type of mental or physical act, often occurring more frequently than what is typically expected. To an outside observer, it may not be clear whether a person engaging in repetitive behaviors has autism, OCD, or no diagnosis at all. However, what distinguishes them is the person’s understanding of these behaviors.
Among autistic folks, these behaviors may be vocal (e.g. humming, scripting movie lines or song lyrics) or motoric (e.g., arm flapping, body rocking, lining up items/objects). While the purposes of these actions vary by the individual, they are generally practiced to meet some kind of need. For instance, an autistic person might be seeking some type of sensory stimulation or reacting to a social situation, often called stimming.
Repetitive behaviors in OCD often involve an excess amount of otherwise common behavior, such as locking doors or washing hands. Whereas a person without OCD might do these things automatically, an individual suffering from OCD may spend several minutes or even hours engaging in these behaviors. Unlike repetitive behavior in autism, OCD compulsions occur as a means to reduce distress. While these excessive behaviors may be in response to a particular obsession, they can also be entirely unrelated.4
Obsessions
Obsessions are typically recurrent and persistent, meaning they can become preoccupying for someone, and make it difficult to focus on other things. Obsessions can take up a great deal of mental energy, resulting in inflexibility and exhaustion.
Obsessive thinking most commonly seen in autistic people typically involves highly preferred topics. One of the key diagnostic indicators for autism involves restricted interests and activities, meaning that these individuals are more likely to be consumed by their fascinations, and it is common for an autistic person to become a true expert in any given area.1
Conversely, people with OCD experience obsessions as being far more distressing and unwanted. The anxiety or sense of dread resulting from such thoughts, urges, or mental images can be consuming, sometimes resulting in an OCD attack. Examples include a person feeling responsible for something bad that happened or having concerns about perfection. Importantly, these thoughts are distinguished from everyday preoccupation by how intrusive and time-consuming they become.
Thought Rigidity & Inflexibility
Rigid thinking involves the inability or unwillingness to modify one’s thoughts or beliefs, even in the presence of contrary evidence. It is quite common, and indeed appropriate, to hold on to certain personal concepts as these reflect one’s values. However, for those with autism and OCD, this rigidity can cause difficulties adapting to new situations or learning new skills.
Rigidity for autistic folks often involves some difficulty generating more than one solution to a problem (often referred to as “black and white” thinking). This quality, which can be a strength in many contexts, is sometimes viewed negatively as stubbornness. Other forms of rigidity may involve a very literal understanding of the world and social interactions. This can make certain things feel harder, such as using context clues to infer others’ meaning.
Thought rigidity common in OCD can refer to challenges with accepting alternate ways of performing actions or routines.7 Specifically, these individuals may feel unable to change a compulsive routine (e.g. checking that the door is locked four times in a minute) to one that achieves the same objective more realistically (e.g. checking that the door is locked once).
Social Difficulties
Social challenges are common in people with Autism and OCD, and both populations might experience increased anxiety in social situations. Having difficulty relating to others in social interactions and expressing your thoughts and feelings are also commonly experienced by people with either diagnosis.
Moreover, thoughts and behaviors related to OCD can interfere with social functioning, making it difficult to form friendships or keep a job.
Issues With Sensory Processing
Sensory processing issues are common in both Autism and OCD. Research has found that sensory processing sensitivities in childhood are linked with OCD symptoms later in life.8 This was particularly true for oral and tactile hypersensitivity. It is thought that intolerance to sensory stimuli contributes to ritualistic behavior in children with OCD.9
Sensory issues are very common for people with Autism, and are even a part of the diagnostic criteria. People with Autism can experience hypersensitivity (over-responsiveness) to sensory stimuli, including sounds, lights, smells, tastes, touches, movements, and others, or they may experience hyposensitivity (under-responsiveness). Sensory overload can occur when a stimulus overwhelms a person’s ability to cope, which can feel like intense anxiety.10
Difficulty Functioning Day-to-Day
A person with OCD may struggle with daily functioning, but for different reasons than are common for a person with Autism. With OCD, thoughts and rituals can become so time-consuming and emotionally overwhelming that the person is unable to carry out their daily responsibilities. This often feels burdensome and discouraging to the person with OCD.
Autism can impair daily functioning in a variety of ways, depending on the individual. The term “spectrum” associated with Autism Spectrum Disorder refers to the wide range of symptoms and severity that people with Autism can experience. Communication difficulties, deficits in organizational skills, fine and gross motor development, and other challenges related to Autism can affect a person’s ability to function at home, work, and school.
What is the best therapy for OCD?
Exposure And Response Prevention Therapy (ERP) – Do live video sessions with a therapist specialized in ERP, the gold standard treatment for OCD. Treatment from NOCD is covered by many insurance plans. Start With A Free 15 Minute Call
Key Differences Between OCD and Autism
Although OCD and Autism may present similarly, they have a distinct difference – while OCD is a mental health disorder, Autism is a neurodevelopmental disorder. Many people with Autism embrace their neurodiversity as simply another way of being in the world.
Other differences between OCD and Autism include:5
- People with OCD often experience distress as a result of their symptoms, while people with Autism do not.
- While people with Autism might feel that their obsessions enhance their lives and bring enjoyment, people with OCD experience decreased life enjoyment as a result of their obsessions and compulsions and most often wish to do away with them.
- People with Autism also exhibit a number of social, linguistic, and cognitive differences that people with OCD do not have.
- Autism is something a person is born with, while OCD can develop at any point in a person’s lifetime.
OCD Vs. Autism Chart
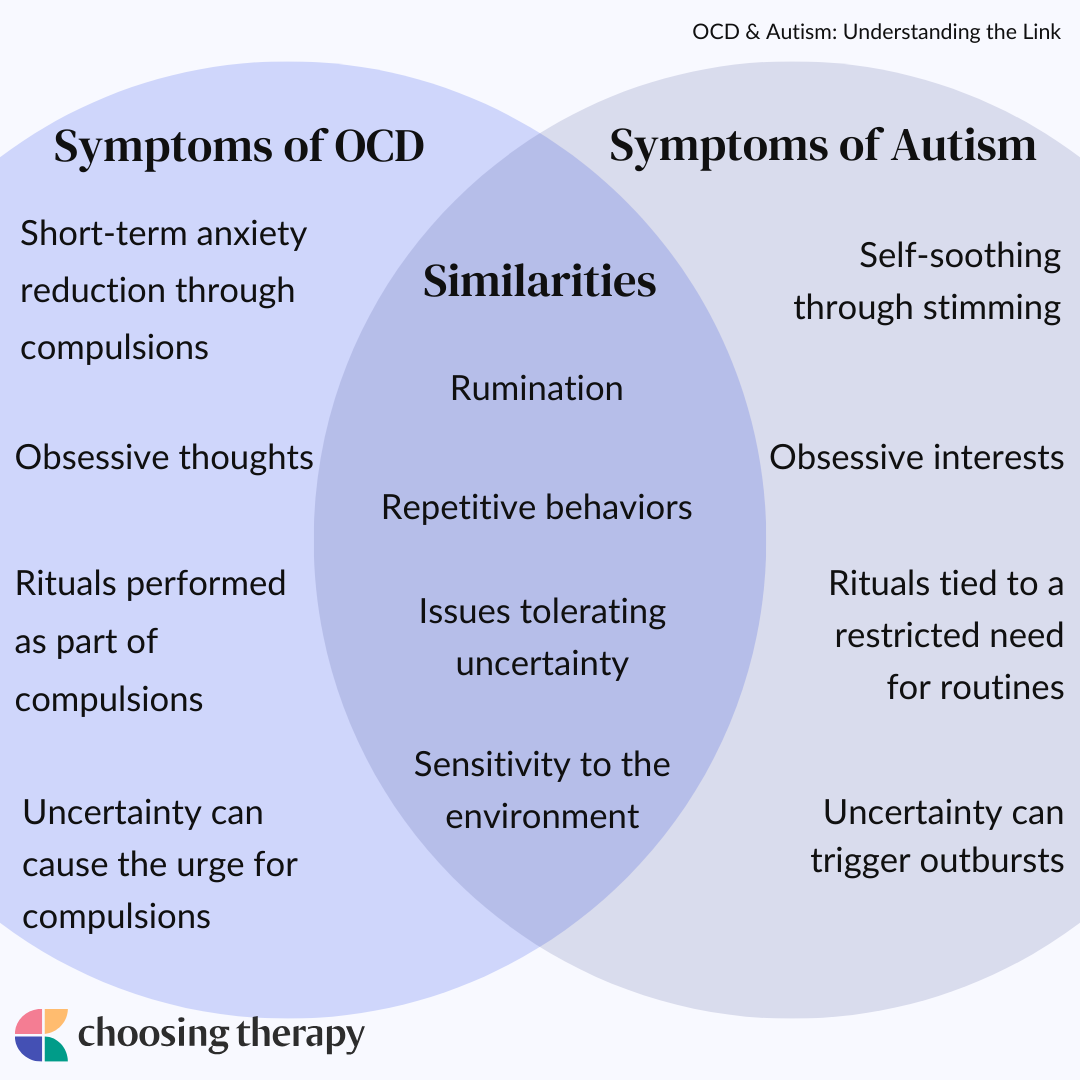
| Symptoms of OCD | Symptoms of Autism | Similarities |
|---|---|---|
| Short-term anxiety reduction through compulsions | Self-soothing through stimming | Repetitive behaviors |
| Obsessive thoughts | Obsessive interests | Both may contain rumination on the same material, but those with autism derive pleasure from their obsessive interests while those with OCD have distress from obsessions |
| Rituals performed as part of compulsions | Rituals tied to a restricted need for routines | Repetitive rituals |
| Uncertainty can cause the urge for compulsions | Uncertainty can trigger outbursts or extreme emotional responses | Issues with tolerating uncertainty and doubt |
| Having increased obsessions around social interactions, or intrusive thoughts following the social interaction | Hyper-focusing on a certain interest during social interactions, lack of understanding social cues, sometimes issues with verbalization | Issues with social interaction |
| Possible triggers to OCD symptoms through sensory input | Easily overstimulated by lights, sounds, or other stimuli not easily processed by the brain | Sensitivity to environment, or issues with sensory input |
Can You Have OCD and Autism?
It is fairly common for autistic individuals to be diagnosed with a secondary psychiatric disorder, with up to 80% having at least one comorbidity.11 In one study, OCD was reported to co-occur with autism in 37% of the population.12 More specifically, autistic people are twice as likely to receive a diagnosis of OCD, while those with OCD have a four times higher risk of a later autism diagnosis.13
While there are many similarities between the intrusive thoughts and compulsive behaviors attributed to people with OCD and the repetitive patterns of behavior among autistic individuals, they are not identical. Importantly, the most reported differences between the two populations involve the person’s subjective experiences of these thoughts and behaviors.
Do OCD and Autism Have Similar Causes?
Experts are not sure of the exact causes of either OCD or Autism. It is thought that genetics, brain abnormalities, stress, and environmental factors may play a role in the development of OCD. Similarly, researchers think that autism may come from a mix of genetic and environmental factors. Some preliminary research supports some possible shared genetic components between OCD and Autism.13 Especially since the rate of Autism is higher in those with OCD than in the general public, experts are curious about similar genetic pathways.13
How Are Autism & OCD Diagnosed?
Autism and OCD are diagnosed by trained professionals using a standardized set of criteria outlined by the DSM-5. There are currently no medical tests that can identify either disorder.
Autism can sometimes be diagnosed as early as age two. In young children, medical professionals monitor specific developmental milestones such as playing, speaking, and learning new things to see if a child is on an expected trajectory. If such developments are delayed, a family may receive a referral to other healthcare professionals for additional screening. Typically, regardless of the age of the individual, a diagnostic evaluation for autism involves assessments of cognitive and language abilities, an observation of their behavior, and a structured interview with caregivers about their concerns.
OCD can also be diagnosed at almost any age, though young children may have difficulty articulating the nature of some of their thoughts or behaviors. A trained mental health professional will conduct a thorough psychological evaluation in order to provide a diagnosis of OCD. A referral for a physical exam might also be recommended in order to rule out any organic causes for the symptoms.
Are OCD Diagnoses More Commonly Missed in Those With Autism?
Autism and OCD share many symptoms, making it difficult to correctly diagnose.14 A recent study found that OCD is a common misdiagnosis in children who grow up to be diagnosed with Autism later in life.15 Someone with both OCD and Autism may have their symptoms attributed to only one diagnosis.
An experienced clinician will be able to tease apart these symptoms to provide a correct diagnosis through a comprehensive assessment. The key differences between Autism and OCD, including how a person feels about their obsessions and ritualistic behaviors, and viewing the person’s story through a developmental lens, will aid the clinician in arriving at the most fitting diagnosis.
How to Treat OCD in Autism
Autism is not a condition that necessarily requires intervention. Many autistic folks can live perfectly happy lives with minimal or no support. However, there may be certain challenges associated with an autism diagnosis that can be the focus of various types of treatment. If an autistic person also has OCD, it is likely that they will need the help from one or more trained mental healthcare professionals.
Therapy for OCD
Treatment for OCD typically involves helping patients to gain insight into their obsessions and compulsions. ERP for OCD is one of the most frequently-used interventions, which involves exposing patients to challenging situations while discouraging them from engaging in compulsive behavior.16 This work is often conducted by a psychologist or therapist with specialized training in ERP and OCD.
Medication
As many as 64% of autistic children with comorbid conditions may be prescribed at least one medication throughout treatment.17 To address repetitive behaviors and anxiety, the most commonly prescribed class of medications for autistic children are serotonin selective reuptake inhibitors (SSRIs).
SSRIs are generally thought to be safe, with low side effect profiles and have some demonstrated effectiveness in reducing obsessive compulsive symptoms in children and adolescents without autism.18
Treatment for OCD
NOCD: Online OCD Treatment Covered by Insurance – Regain your life from OCD. Do live video sessions with a licensed therapist specialized in treating OCD. Treatment from NOCD is covered by most major insurance plans. Learn how you can use your insurance benefits. Visit NOCD
Talkiatry: Is OCD Medication Right for You? Speak with a Doctor – Talkiatry can match you with a psychiatrist who takes your insurance and is accepting new patients. They’re in-network with major insurers and offer medication management with supportive therapy. Free Assessment
How to Cope With OCD as an Autistic Person
Learning to cope with behaviors like obsessions and compulsions can be a challenge, regardless of whether there are comorbid diagnoses. These behaviors can range from mildly annoying to significantly interfering, and so it might be hard to know where to start. However, there are some steps you can take to help you cope throughout treatment.
Below are some ways to cope with OCD and autism:
- Challenge yourself: Try gradually challenging yourself to tolerate difficult situations while not engaging in compulsive behavior. This can help you slowly ease yourself into new patterns of behavior and thinking.
- Seek support: It is extremely important to identify a support system, such as family members, friends, or support groups, who can help you work towards your goals. This process of change can be difficult, requiring support and encouragement from loved ones.
- Seek treatment: Effectively treating OCD involves modifying one’s lifestyle with support of a therapist in order to minimize avoidance and actively challenge obsessive thoughts and behaviors.
In My Experience
Repetitive and ritualistic behavior in autism can look quite similar to compulsions in OCD. Behavioral treatments have been found to be effective in addressing these symptoms, but individual differences may make some strategies more effective than others. While there can be considerable overlap between diagnoses, the factor most relevant for treatment involves the level of distress that the individual feels about their thoughts and behaviors.

OCD & Autism Infographics
ChoosingTherapy.com strives to provide our readers with mental health content that is accurate and actionable. We have high standards for what can be cited within our articles. Acceptable sources include government agencies, universities and colleges, scholarly journals, industry and professional associations, and other high-integrity sources of mental health journalism. Learn more by reviewing our full editorial policy.
-
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
-
Zandt, F., Prior, M., & Kyrios, M. (2007). Repetitive behavior in children with high functioning autism and obsessive compulsive disorder. Journal of Autism and Developmental Disorders, 37(2) 251-259. https://doi.org/10.1007/s10803-006-0158-2
-
Lord, C., et al. (2018). Autism spectrum disorder. Lancet, 392 (10146). 508-520. https://doi.org/10.1016/s0140-6736(18)31129-2
-
Stein, D. J., et al. (2019). Obsessive–compulsive disorder. Nature Reviews Disease Primers, 5(1). https://doi.org/10.1038/s41572-019-0102-3
-
National Institute of Mental Health. (2022). Obsessive-Compulsive Disorder. Retrieved from https://www.nimh.nih.gov/health/topics/obsessive-compulsive-disorder-ocd
-
Mayo Clinic. (2018). Autism Spectrum Disorder. Retrieved from https://www.mayoclinic.org/diseases-conditions/autism-spectrum-disorder/symptoms-causes/syc-20352928
-
Whitton, A.E., Henry, J.D., & Grisham, J.R. (2014). Moral rigidity in obsessive compulsive disorder: do abnormalities in inhibitory control, cognitive flexibility, and disgust play a role? Journal of Behavior Therapy and Experimental Psychiatry, 45, 152-159. http://dx.doi.org/10.1016/j.jbtep.2013.10.001
-
Dar, R., Kahn, D. T., & Carmeli, R. (2012). The relationship between sensory processing, childhood rituals and obsessive-compulsive symptoms. Journal of behavior therapy and experimental psychiatry, 43(1), 679–684. https://doi.org/10.1016/j.jbtep.2011.09.008
-
Hazen, E. P., Reichert, E. L., Piacentini, J. C., Miguel, E. C., do Rosario, M. C., Pauls, D., & Geller, D. A. (2008). Case series: Sensory intolerance as a primary symptom of pediatric OCD. Annals of clinical psychiatry : official journal of the American Academy of Clinical Psychiatrists, 20(4), 199–203. https://doi.org/10.1080/10401230802437365
-
Balasco L, Provenzano G, Bozzi Y. Sensory abnormalities in autism spectrum disorders: a focus on the tactile domain, from genetic mouse models to the clinic. Front Psychiatry. 2019;10:1016. doi:10.3389/fpsyt.2019.01016
-
Kose, L. K., Fox, L., & Storch, E. A. (2017). Effectiveness of Cognitive Behavioral Therapy for Individuals with Autism Spectrum Disorders and Comorbid Obsessive-Compulsive Disorder: A Review of the Research. Journal of Developmental and Physical Disabilities, 30(1), 69–87. https://doi.org/10.1007/s10882-017-9559-8
-
Joshi, G., et al. (2010). The Heavy Burden of Psychiatric Comorbidity in Youth with Autism Spectrum Disorders: A Large Comparative Study of a Psychiatrically Referred Population. Journal of Autism and Developmental Disorders, 40(11), 1361–1370. https://doi.org/10.1007/s10803-010-0996-9
-
Meier, S.M., et al. (2015). Obsessive compulsive disorder and autism spectrum disorders: longitudinal and offspring risk. Plos One. https://doi.org/10.1371/journal.pone.0141703
-
Pazuniak, M., & Pekrul, S. R. (2020). Obsessive-Compulsive Disorder in Autism Spectrum Disorder Across the Lifespan. Child and adolescent psychiatric clinics of North America, 29(2), 419–432. https://doi.org/10.1016/j.chc.2019.12.003
-
Rødgaard, E. M., Jensen, K., Miskowiak, K. W., & Mottron, L. (2021). Childhood diagnoses in individuals identified as autistics in adulthood. Molecular autism, 12(1), 73. https://doi.org/10.1186/s13229-021-00478-y
-
Edelstein, M.L. & Lenfestey, S.P. (2023). Treatment of socially mediated compulsive behavior in a high functioning adolescent with autism spectrum disorder. Education and Treatment of Children, 9(1), 1-5
-
Spencer, D., et al. (2013). Psychotropic medication use and polypharmacy with children with autism spectrum disorders. Pediatrics, 132, (5), 833-840. https://doi.org/10.1542/peds.2012-3774
-
King, B. H., et al. (2009). Lack of Efficacy of Citalopram in Children With Autism Spectrum Disorders and High Levels of Repetitive Behavior. Archives of General Psychiatry, 66(6), 583. https://doi.org/10.1001/archgenpsychiatry.2009.30

We regularly update the articles on ChoosingTherapy.com to ensure we continue to reflect scientific consensus on the topics we cover, to incorporate new research into our articles, and to better answer our audience’s questions. When our content undergoes a significant revision, we summarize the changes that were made and the date on which they occurred. We also record the authors and medical reviewers who contributed to previous versions of the article. Read more about our editorial policies here.
Author: No Change
Reviewer: No Change
Primary Changes: Updated for readability and clarity. Reviewed and added relevant resources. Added “OCD Vs. Autism Chart”,
“Do OCD and Autism Have Similar Causes?”. New material written by Michelle Risser, LISW-S and reviewed by Kristen Fuller, MD.
Author: No Change
Reviewer: No Change
Primary Changes: Updated for readability and clarity. Reviewed and added relevant resources. Added “OCD Vs. Autism: Key Differences”, “Is OCD a Form of Autism?”, “Social Difficulties”, “Issues With Sensory Processing”, “Difficulty Functioning Day-to-Day”, “Are OCD Diagnoses More Commonly Missed in Those With Autism?”. New material written by Heather Artushin, LISW-CP and reviewed by Kristen Fuller, MD.
Author: Matthew Edelstein, Psy.D, BCBA-D
Reviewer: Heidi Moawad, MD
Your Voice Matters
Can't find what you're looking for?
Request an article! Tell ChoosingTherapy.com’s editorial team what questions you have about mental health, emotional wellness, relationships, and parenting. Our licensed therapists are just waiting to cover new topics you care about!
Leave your feedback for our editors.
Share your feedback on this article with our editors. If there’s something we missed or something we could improve on, we’d love to hear it.
Our writers and editors love compliments, too. :)
Additional Resources
To help our readers take the next step in their mental health journey, ChoosingTherapy.com has partnered with leaders in mental health and wellness. ChoosingTherapy.com is compensated for marketing by the companies included below.
OCD Therapy
NOCD: Effective, Affordable, & Convenient OCD Therapy Do live, face-to-face video sessions with a therapist who specializes in treating OCD and get 24/7 support between sessions. NOCD is covered by many insurance plans and is available nationwide. Visit NOCD
Treatment from an Online Psychiatrist
Talkiatry OCD is treatable. Talkiatry specializes in OCD and provides personalized care with medication and additional support. Get started with a short assessment.
OCD Newsletter
A free newsletter from the experts at ChoosingTherapy.com for those impacted by OCD. Get helpful tips and the latest information. Sign-Up

Best OCD Therapy Online
To find the best online OCD therapy, our team reviewed over 50 providers. Many of these options accept insurance, prescribe medication, and provide peer- or therapist-led OCD support. The best, NOCD, offers evidence-based treatment from specialists, providing Exposure and Response Prevention (ERP) therapy for OCD and its many subtypes.
Best Online OCD Resources
We evaluated numerous online OCD resources and treatment options to bring you our top recommendations. These platforms, apps, and podcasts provide trustworthy information and support, whether through peer communities or expert guidance. Whether you’re looking for therapeutic options, medication management, or education, this list – compiled by a clinical psychologist – will meet your needs.
